














 14 / 24
14 / 24

Page 14
— Health Care Properties Quarterly — July 2017
www.crej.comTechnology
Blending Form into the Function of Your
Healthcare Facility
1660 Lincoln Street, Suite 100
l
Denver, CO 80264
l
303.861.4800
l
www.TPS.designExperts in Design Mixology
I
t’s no secret that technology’s
role in health care is increas-
ing and evolving with every
passing day. Meanwhile, with
the exception of building
information modeling and vari-
ous mobile technologies, buildings
are mostly being built in the same
manner as they were 10 to 20 years
ago. Technology and low-voltage-
related systems used to be an after-
thought because of their minimal
impact on the building operations
and systems. Take, for example, an
ultra-high-tech computer chip fac-
tory built in Denver in the 1980s. At
that time, it embodied some of the
latest technology. However, the fac-
tory had three low-voltage systems:
access control, video surveillance
and fire management. A factory of
this complexity today could poten-
tially have more than 30 systems to
operate various controls, security,
sensors and other systems.
The industry often references
“MEP” as mechanical, electrical and
plumbing due to the intense nature
of these scopes and considering
they range from 30 to 40 percent of
most health care project budgets.
Given the growing cost and need for
low-voltage technology, soon “MEP”
will be known as “MEP-T” with the
technology network as the fourth
crucial utility.
Health care organizations are
investing less in mega projects
and more on infrastructure and
technology (as well as outpatient
and physician integration). Many
renovation and expansion projects
are experiencing the challenges of
interfacing with existing low-volt-
age infrastructure
or implementing
entirely new infra-
structure. A health
care provider must
consider the cost-
benefit analysis
of salvaging exist-
ing infrastructure
or building new
infrastructure to
accommodate the
rapidly advancing
technology sys-
tems.
Historically, low-
voltage systems
have been provided by specialty
subcontractors that work under-
neath electrical, mechanical, secu-
rity and door subcontractors. These
scopes of work often are executed
in a silo. However, if these systems
are not carefully integrated from
the beginning of the project, an
influx of low-voltage coordination
and clash issues will surface. These
late-coordination issues typically
increase project cost and schedule
during installation, commission-
ing and turnover. Considering all
systems in an MEP-T approach can
minimize these clashes and solve a
problem before it becomes one.
Through research and project
results, we have found that an
MEP-T integrated approach to deliv-
ering low-voltage systems during
construction can save roughly 8 to
27 percent, depending on project
complexity. Low-voltage systems
are becoming an increasingly valu-
able portion of the overall project
budget. Based on 10 health care
projects across the country, low-
voltage accounted for roughly 5 to
10 percent of the overall budget, so
savings are significant.
How to Approach the Fourth Utility
For all health care organizations
beginning new projects, the T in
MEP-T should be just as much of a
discussion topic in the schematic
design phase as the structure and
envelope. Facility operators will
need time to thoroughly assess
their infrastructure, understand
evolving and available medical tech-
nology, review technology matrix
dependencies and predict future
growth of the facility.
JE Dunn has taken a fully inte-
grated approach to incorporating
network systems prior to construc-
tion commencing on several proj-
ects, the Banner Harmony Hospital
in Fort Collins and at the St. Joseph
Catholic Health Initiative Replace-
ment Hospital in Dickinson, North
Dakota. Both large-scale hospitals
(north of $50 million and more than
150,000 square feet) saw the value
in approaching all low-voltage sys-
tems in a comprehensive approach,
as the fourth utility of the hospital.
The project team should properly
account for these technology con-
siderations early in the budgeting
and construction planning. Early
emphasis placed on technology will
help vet coordination challenges
up front and reduce downstream
issues and increased costs.
Teams should be asking questions
related to interoperability for central
MEP-T: Network technology as the fourth utilityPaul Boucher
Director of
systems integrated
solutions, JE Dunn
Construction,
Denver
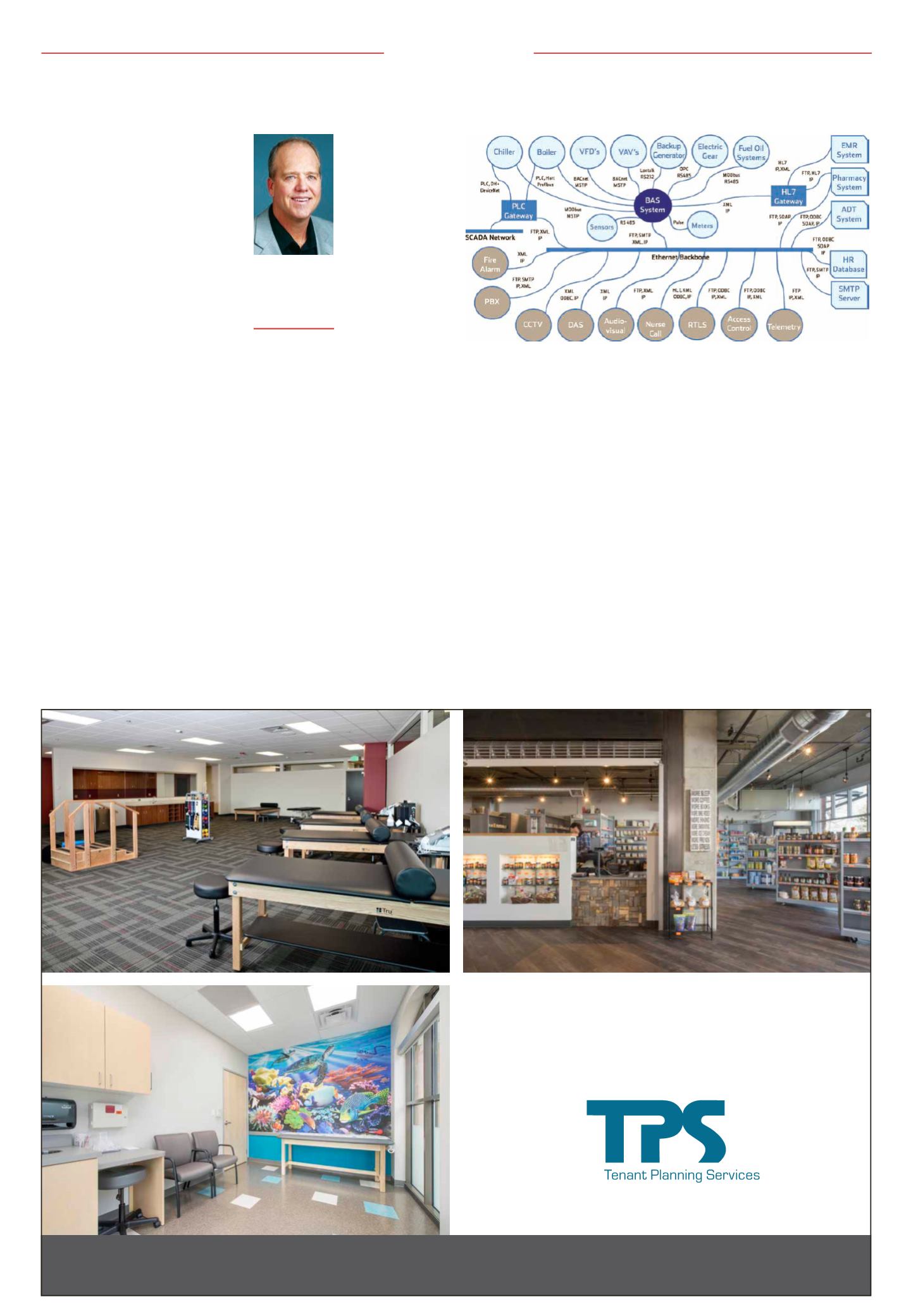
The figure shows an example of a protocol mapping one-line diagram that describes vari-
ous technology systems and provides physical, network and application layer protocols in a
simple but effective communication tool for the team members to understand.
Please see ‘Boucher’ Page 23