














 60 / 76
60 / 76

Page 12B—
COLORADO REAL ESTATE JOURNAL
—
March 4-March 17, 2015
A
s health care practices
change, the real estate
that houses those
practices must either adapt to
accommodate modern practices
or risk becoming obsolete. In
the 1960s, the most frequently
occurring physician practice
involved a sole provider,
one nurse and possibly one
receptionist. This practice type
easily fit into 700 to 900 square
feet.
Today, most practices include
multiple providers, medical
assistants, nurse practitioners
and support staff. Even small
practices are now pushing the
3,000-sf mark and it is very
common to have significantly
larger offices.
Many medical office buildings
constructed in the 1970s and
1980s have reached a distressed
state. The buildings need
significant capital infusions
in order to keep up with the
modern health care practice.
What are the key factors
for an existing medical office
building that would allow it to
be repositioned and become
viable well into the future?
There are several key factors
to consider when evaluating a
turn-around versus a scrape and
redevelop project. Perhaps the
most critical consideration is
whether the building allows for
assembling large blocks of space
while continuing to meet exiting
requirements. If it is not possible
to assemble 3,000- to 7,000-sf
spaces, it is probably not worth
considering additional capital
investment in the property.
From there, it is important to
consider what factors led to the
building becoming challenged.
Did the market change or did a
hospital move? If so, there may
not be the demand to support
the medical building, even with
capital investment.
Other factors to consider
include sufficient parking (five
spaces per 1,000 sf), availability
for high-capacity data (T1 lines
are no longer sufficient for most
practice needs), power capacity
and distribution that is sufficient
to handle the needs of a modern
practice (dedicated 100-amp
subpanels have become quite
common for most practices).
Assuming you have a
medical building that passes
the considerations above,
it may be worth a capital
investment. By treating the
project as a redevelopment with
consideration and effort put
toward replacing key building
systems – such as the heating,
ventilating and air-conditioning
system, performing an elevator
modernization, or replacing
dated lighting with modern
light-emitting diode fixtures – a
thorough and complete cosmetic
renovation to eliminate all traces
of the 1970s and 1980s design
choices can position the building
to be competitive with new
construction.
In addition to the high-quality
renovation of existing building
systems and common areas, it
is important to be adequately
capitalized to provide sufficient
tenant improvement allowances
for tenants to convert dated,
small spaces into modern, large,
properly flowing medical office
spaces. Frequently allowances in
excess of $45 and $50 per sf are
required. It is not uncommon
for spaces to require a complete
gut and remodel. Similarly, life-
safety systems may be insufficient
to meet current codes and may
require significant upgrades.
In order to retain current
tenants, one great opportunity
that frequently exists in these
buildings is to reduce operating
expense. The combination of
replacing light fixtures and
HVAC systems can greatly
reduce power requirements
and maintenance services.
This reduction in cost can be
captured by the landlord in
terms of increased net rental
rates while holding the overall
gross rental-cost structure to the
tenant in line with market rental
increases.
While a renovated building will
never quite meet the standards
of brand new construction,
it is possible to deliver a well-
renovated, highly functional
medical office building that
is likely within 20 percent of
the quality and style of a new
building. The opportunity
comes in redeveloping existing
buildings with the acquisition
price for 50 to 60 percent of
the cost of new construction.
Completing a high-quality
renovation can frequently lead to
a rental rate that is effectively 10
to 12 percent on the cost.
Working through the
renovations, aggregation of
contiguous space, operating
expenses and tenant
improvements should yield a
stabilized building within two
to three years. If the renovated
project is successful attracting
national credit tenants, the
stabilized asset can command
prices between a 7 and 8 percent
capitalization rate. All of these
factors combine to yield a mid-
20s to low-30s internal rate of
return employing little to no
leverage.
Bank financing is not generally
available in large amounts for
these kind of medical office
turnaround projects. It is
very possible to obtain bank
improvement credit facilities
that largely fund the tenant
improvements as the project
leases up. Bridge financing can
be obtained usually for 50 to 60
percent of the project cost with
rates of 8 to 11 percent. Bridge
financing certainly can erode
returns if the leasing schedule is
delayed. For the most part, the
redevelopment project needs to
rely on significant equity until
the property has been stabilized.
Assuming the “bones” of
medical office buildings from
the 1970s and 1980s are in
good shape, these buildings do
not need to become obsolete.
Many dated medical buildings
can be resurrected and provide
functional and cost-effective
space for the practices of today.
O
ver the past seven
months, I have been
on a journey into
the world of integrated project
delivery for a new 142-bed
hospital in Henderson, Nevada.
According to the AIA, IPD is
a project delivery approach
that integrates people, systems,
business structures and practices
into a process that collaboratively
harnesses the talents and insights
of all participants to optimize
efficiency through all phases
of design, fabrication and
construction.
In my 18 years of providing
interior design for health care
environments, this was my fist
IPD experience. I was excited
to provide design in a new
and more efficient way. One
can’t describe IPD without lean
principles involved, which for an
“Achiever Type A personality” is
inspiring.
If there is one nugget of
information that I can share
with the design and construction
community, it would be about
the benefits of “pull planning.”
The Lean Construction Institute
defines “pull” as a method
of advancing work when the
next-in-line customer is ready
to use it. A “request” from the
customer signals that the work
is needed and is “pulled” from
the performer. Pull releases work
when the system is ready to use
it. LCI defines “planning” as “the
act of conversation that leads to
well-coordinated action.”
The project team meets
every Wednesday in what we
fondly call The Big Room for
a full day of constant dialogue
and information sharing.
After introductions, rules of
engagement and hot topics,
we stand up and head to the
40-foot pull plan board. The
board has weeks labeled along
the top, starting with the current
day or week on the left and
expanding out two months
to the right. Below the dates,
running horizontally, are swim
lanes for each trade partner,
including architect, mechanical,
electrical, interiors, structural,
site, constructor and owner, each
trade with different colored
sticky notes populating the lanes.
Pull planning is working
backward from a target
completion date (milestone).
Tasks are defined and sequenced
so that their completion releases
work. When our project team
is pull planning, we start
downstream with a specific task,
event or deliverable, and work
backward to current date with
each of us asking, “What do I, as
a customer, need from others in
order to meet my commitment
to the milestone?”
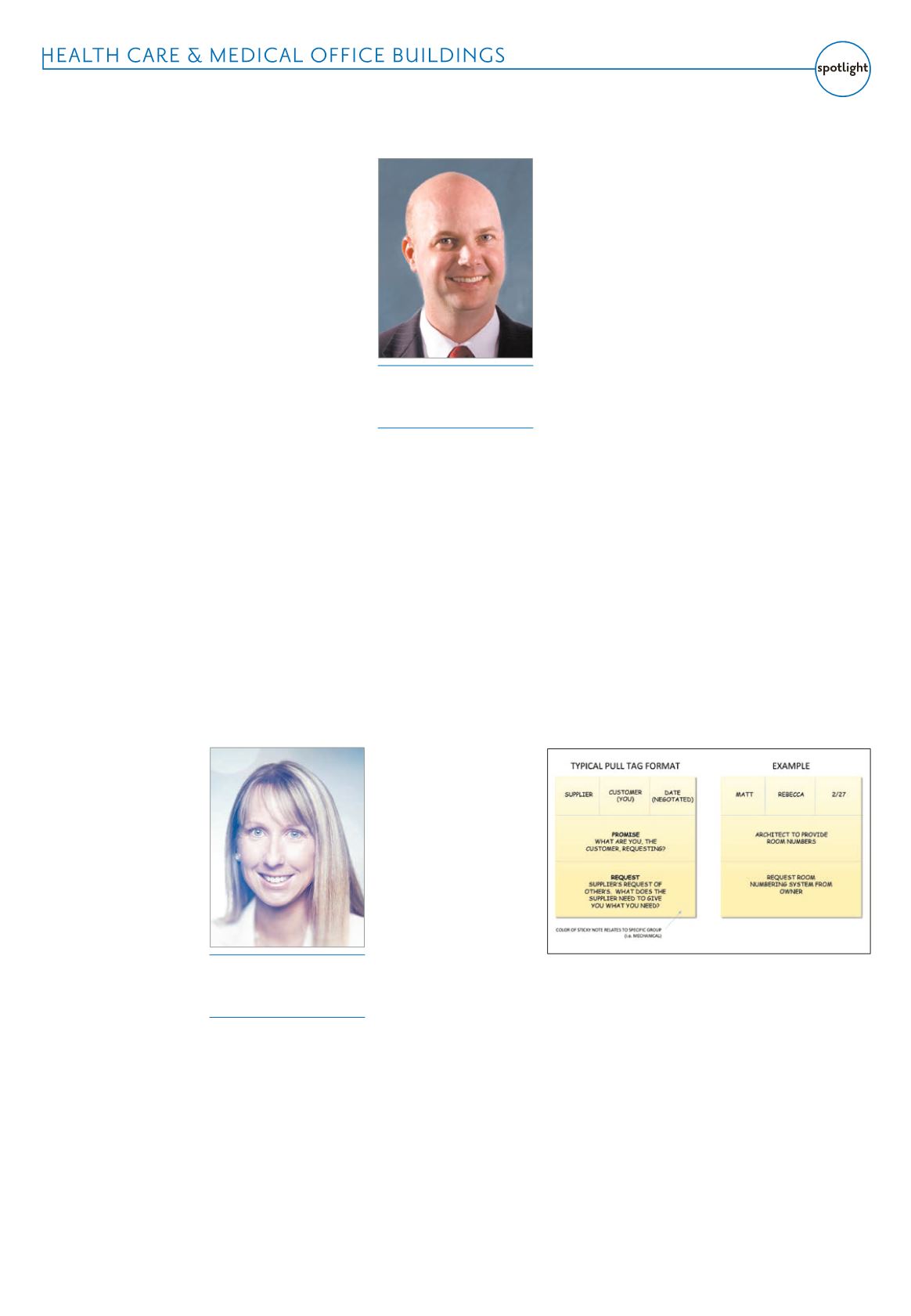
If I have a need, it is requested
on a sticky note and placed in
the swim lane of the supplier.
Before I place the request on
the board, a conversation is
had between the customer
and the supplier, which creates
understanding, commitment
and agreement. Both parties
negotiate the due date. This pull
tag may result in the supplier
becoming a customer for a need
from another supplier.
Pull planning is an effective
technique for outlining and
meeting scheduling deadlines
for construction projects. When
handled correctly, pull planning
eliminates miscommunications
and allows every key player to
be integrally involved in the
planning process. There are key
components to successful pull
planning:
1. Define the phasing of work
(milestone) and determine
completion dates for the
phases.
Go to the pull plan
board with a purpose and a
focused task at hand. A team
cannot work backward if they do
not know what the deliverable is
or the date needed.
2. Have the right people
present.
Typically a single
activity, event or deliverable is
the focus of a pull-planning
event, so having all key trade
partners who have a stake or
a share in the final deliverable
is key. A customer can’t write
a request, assign the supplier
and give a date if the supplier
is not present. The risk is that
the supplier may not be aware
of the request made of them,
fully understand the request or
may not be able to commit to
the deadline set. Also, having
someone stand in as a substitute
for others runs a risk because the
conversation surrounding the
request and commitment cannot
be completely understood unless
the stakeholders are present.
3. Promote a global
understanding.
Everyone needs
to thoroughly understand the
work, not just their own scope of
work, but also the scopes of work
of other trades. Why? Because on
a construction project the various
trades are interdependent on
one another, and each individual
must know the preceding and
succeeding trades to contribute.
When done correctly, pull
planning is very effective
at meeting milestones. Pull
scheduling often will expose the
need for smaller batches, just in
time delivery, improved leveling
of resource and reduced lead
times. Workflow becomes more
reliable and efficient as the waste
of waiting, redundancy and
overprocessing are eliminated.
These are all characteristics of a
growing lean culture.
If you ever have an opportunity
to initiate or participate in an
IPD project, I highly recommend
it. Our firm has internalized the
concepts and process to become
more efficient and effective at
what we do and are striving to
build a lean culture. Face it, who
doesn’t want to remove waste
from their work and daily lives?
Considerations for medical building repositioning Designing a hospital with integrated project deliveryJames C. Turpen
CEO, Centum Health
Properties Inc., Denver
Rebecca Brennan
AAHID President-elect, associate
principal, Gallun Snow, Denver
Pull plug diagram